Colectomy
Introduction
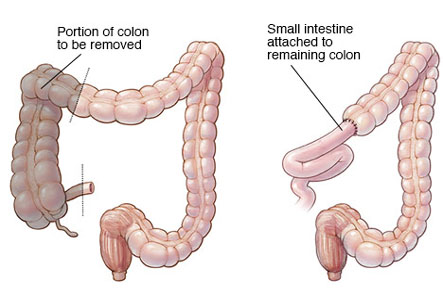
Colectomy is an operation that involves removal of whole or part of the large intestine. It is usually undertaken in patients who have an inflammatory condition of the intestine like Ulcerative Colitis or Crohn’s disease or benign or cancerous tumors in the colon.
As with other surgeries Colectomy is also associated with risks of infections, bleeding, pain, and injury to the small intestine, bladder or blood vessels. Apart from this there are small risks associated with general anesthesia like heart attack or stroke.
Alternative to total Colectomy is Partial Colectomy that involves removal of part of the large intestine. Steroids and other drugs effective in inflammatory bowel diseases may be a non surgical alternative.
colon, also called large intestine, is a long tubelike organ at the end of digestive tract
Once the laparoscope is inserted through this opening four to five other small key hole incisions are made over the sides of the abdomen.
Before the surgery is undertaken a general health checkup is mandatory. You will need to be empty stomach for 6 to 8 hours before the surgery. Usually a light dinner is recommended. Food or water in the stomach when under anesthesia can go into your lungs and may even cause death.
Once inside the operation theatre an intravenous line will be made in one of the veins of your fore arm. You may be given medications to allay anxiety before the operation. Instruments to monitor your heart rate, rhythm (using EKG), blood pressure and oxygen saturation (to detect adequacy of breathing) will then be plugged in. Usually general anesthesia is advocated for Colectomy wherein you will be unconscious and pain free during the operation. The abdomen is cleaned and sterile surgical drapes are placed over it.
Surgery Procedure
Once you are made unconscious a small 5-10mm cut is made just below your navel. The laparoscope is a thin telescope like instrument with a camera on its tip that transmits images to a monitor in the operating room. Your surgeon will be guided through the operation through these images. Your abdomen is inflated with carbon dioxide through the first nick. This will allow room for maneuvering the instruments. Once the laparoscope is inserted through this opening four to five other small key hole incisions are made over the sides of the abdomen. Surgical instruments will be inserted through these incisions.
Once inside the whole of the colon is identified. The colon starts from the ileum and ends at the rectum. This is nearly five feet long. The blood vessels over the section of colon to be removed will be clipped off. The stumps at the ileum and rectum are then identified and freed from their membranous attachments in the abdomen.
Then a snare like instrument with a wire loop at its tip is inserted through one of the key hole incisions. This will be used to clip and cut the ends of the colon. The contents of the colon are highly infectious and any spillage may result in infections of the whole abdomen that may be life threatening. For this purpose the cut off segment of colon is placed within a sterile bag inside the abdomen. One of the key hole incisions is then enlarged and the bag containing the tightly clipped colon segment is pulled out of the abdominal cavity. Thereafter the ileal end of the colon is joined with the rectal end with help of special surgical staples.
Once the joining of the stumps of the colon is completed the abdominal cavity is rinsed thoroughly with saline water and the surgeon will check if there is any bleeding. If the joined ends are not closed adequately there may be leakage. Your surgeon will carefully check for leaks before completing the operation. A drainage tube is left in the abdomen to drain out the excess fluids. The abdomen is deflated and the incisions sutured or staples and bandaged.
Post operative considerations
After surgery you will be taken to the recovery room. Here you will be awakened and given pain relieving medications. Once your heart rate, blood pressure and breathing are stabilized, you will be sent to the hospital bed. You will be discharged in around a week’s time. At discharge you can have soft diet excluding raw fruits and vegetables. Drink plenty of water to stay hydrated and to prevent constipation. Avoid lifting heavy weights and strenuous exercise for the first six weeks after surgery.